Penile fracture
Though the condition is referred to as a penile fracture, the penis unsurprisingly does not have a bone!
Aetiology:
-Trauma to the erect penis leading to a break in the continuity of the tunica albuginea overlying the corpora cavernosa.
-Most patients are hesitant to disclose the events leading up to the injury; however, a good history is important in understanding whether this is indeed a penile fracture.
-Commonly noted in 30 - 40-year-old males.
-The break occurs as a result of a significant amount of force during coitus, where the erect penis makes contact with the partner’s perineum or pubis.
-It may also be seen in forceful handling of the penis, as with masturbation or using adjuncts to heighten the male’s sexual stimulation.
-At other times, a male may fall off bed onto an erect penis, and while this is a rare cause of a penile fracture, it can indeed happen.
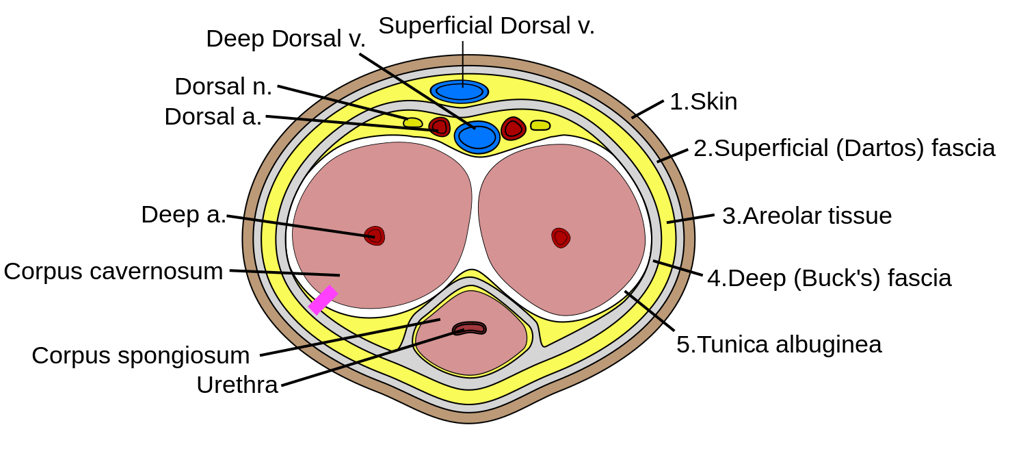
Image 1 - Cross-section of a penis. The pink line indicates the common site of injury, which is the ventrolateral aspect of the right-sided corpus cavernosum.
Assessment:
History - sexual intercourse and impact of the penis followed by a ‘popping or snapping’ sensation or sound, immediate detumescence (loss of erection,) pain and swelling. It is important to check if the patient can void and if there is haematuria, as it may indicate a urethral injury.
Examination - A bruised and swollen penis representing an aubergine. The penis may take on a curve towards the intact side. The right side is more commonly affected.
A palpable haematoma within the shaft may be noted.
Examine the perineum. Any bruising or swelling may be indicative of a perineal haematoma.
Penile fracture is a clinical diagnosis. However, if uncertain, imaging can be requested to confirm before intervention.
Investigations:
Routine blood tests for emergency surgery
Imaging - Ultrasound scan of the penis (operator dependent,) MRI scanning (limited availability but an excellent modality) and cavernosography
Urethrogram - useful in case of suspected urethral trauma
Management:
All penile fractures presenting within a week can be managed acutely. More urgent treatment would be needed if the urethra is implicated.
Adequate analgesia and a cold compress (avoid direct contact with ice)
A circumferential incision followed by degloving the penile skin, evacuation of the clot and primary closure of the defect.
Complications:
Curvature of the penile shaft
Painful erections
Penile paraesthesia
Erectile dysfunction
BAUS consensus on the management of penile fracture:
https://rightdecisions.scot.nhs.uk/media/2q1ai034/baus-consensus-document-for-the-management-of-penile-fracture.pdf
Useful links:
https://teachmesurgery.com/urology/other/penile-fracture/
https://gpnotebook.com/en-gb/simplepage.cfm?ID=x20050914141324832459
Images:
Image 1 - Used under the Creative Commons License with an alteration made (inclusion of a pink line to denote the site of Injury) - Mcstrother, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
UroMate
contact@uromate.com
© 2025. All rights reserved.
Disclaimer: The content on UroMate is intended for educational use by medical professionals only. It does not constitute professional medical advice, clinical guidelines, or a substitute for supervision or training. UroMate is not an official authority and accepts no responsibility for clinical outcomes. This site reflects UK clinical practice and may not apply elsewhere. Users must consult official sources such as NICE, EAU, or NHS protocols. Medical knowledge evolves, and while we strive for accuracy, content may not reflect the latest guidance. Not intended for patients or the general public. By continuing to use this site, you acknowledge and accept these terms.